Analysis by Dr. Joseph Mercola
- January 09, 2024Download PDF
STORY AT-A-GLANCE
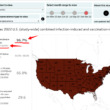
- The latest SARS-CoV-2 variant, JN.1, was first detected in the U.S. in September 2023. By mid-December, it accounted for about half of all COVID cases in the country
- According to the U.S. Centers for Disease Control and Prevention, the rapid spread of JN.1 suggests it may be more transmissible and/or has greater immune-evading abilities
- A vaccinology concept called “immune refocusing” explains how more dangerous viruses can be created by leaky vaccines that do not prevent infection
- By continuing with boosters, we accelerate immune escape. Over time, variants will get better and better at evading our immune responses, and those who keep taking boosters will be the most vulnerable to infection of all
- Because of the mutations seen in JN.1, vaccinologist Geert Vanden Bossche, Ph.D., predicts we will “very soon” see variants that are more virulent but less infectious. If this happens, healthy unjabbed individuals are unlikely to be affected because their first line of defense — their innate immune system — still works as it should. The jabbed, on the other hand, whose innate immune systems have not been trained, and whose adaptive immune systems have become increasingly useless, will be at very high risk of severe complications and death
The latest SARS-CoV-2 variant, JN.1, was first detected in the U.S. in September 2023. By mid-December, it accounted for about half of all COVID cases in the country,1 and calls to get the latest “updated” COVID shot resumed. Cases associated with this variant are also on the rise in the U.K., China and India.2
According to the U.S. Centers for Disease Control and Prevention, the rapid spread of JN.1 suggests it may be more transmissible and/or has greater immune-evading abilities:3
“JN.1 is similar to BA.2.86 but has an additional mutation (L455S) in the spike protein. JN.1 continues to cause an increasing share of infections and is now the most widely circulating variant in the United States.
For the two weeks ending on December 23, 2023, JN.1 is expected to account for 39-50% of all SARS-CoV-2 variants. That’s an increase from the projected prevalence two weeks ago of 15-29%.
We’re also seeing an increasing share of infections caused by JN.1 in travelers, wastewater, and most regions around the globe. JN.1’s continued growth suggests that the variant is either more transmissible or better at evading our immune systems than other circulating variants.”
JN.1 Is Not Associated With More Severe Disease
The CDC does, however, stress that JN.1 does not appear to cause more severe disease than any of the other variants we’ve seen in the last couple of years, most of which have caused nothing more than common cold symptoms. The New York Times even noted:4
“As far as experts can tell, JN.1 does not seem to be causing severe illness in most other people, though even a mild case can still make you feel ‘quite miserable for three or four days,’ Dr. [William] Schaffner [infectious disease specialist at Vanderbilt University Medical Center] said.
The symptoms of a JN.1 infection are similar to those caused by previous COVID variants, including a cough, fever, body aches and fatigue … JN.1 will most likely remain the dominant version of the coronavirus through spring, Dr. Schaffner said.”
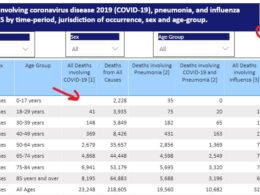
According to data from the British Office for National Statistics, the most commonly reported symptoms among COVID-19 patients in December 2023 included:5,6
| Runny nose (31.1%) | Cough (22.9%) |
| Headache (20.1%) | Weakness or tiredness (19.6%) |
| Muscle ache (15.8%) | Sore throat (13.2%) |
| Trouble sleeping (10.8%) | Worry or anxiety (10.5%) |
Of these, the only symptoms that can be considered “novel” are problems sleeping and worry/anxiety, which could easily be the natural outgrowth of having spent the last four years bombarded with fear-based propaganda about COVID.
Mass Vaccinating During Active Pandemic Is a Disaster
Despite three years of evidence to the contrary, the CDC still insists that existing vaccines are the best way to protect yourself against JN.1. In the video above, vaccinologist Geert Vanden Bossche, Ph.D., discusses the challenges of controlling transmission with vaccines, as even with mRNA technology we’re still chasing the virus.
His resume includes work with GSK Biologicals, Novartis Vaccines, Solvay Biologicals and the Bill & Melinda Gates Foundation. As some of you may recall, in 2021, Vanden Bossche7 published an open letter8 to the World Health Organization in which he warned that implementing a global mass vaccination campaign during the height of the pandemic could create an “uncontrollable monster” where evolutionary pressure will force the emergence of new and potentially more dangerous mutations.
“There can be no doubt that continued mass vaccination campaigns will enable new, more infectious viral variants to become increasingly dominant and ultimately result in a dramatic incline in new cases despite enhanced vaccine coverage rates. There can be no doubt either that this situation will soon lead to complete resistance of circulating variants to the current vaccines,” Vanden Bossche wrote.9
His warning fell on deaf ears, but evidence clearly shows that he was on the right track. Increasingly, variants have mutated to evade both natural and injection-based immunity, with those having received the COVID shots now being at higher risk of infection than their unjabbed peers.Download the Entire Article for FREE
The COVID Jabs Are Driving Potentially Hazardous Mutations
As explained by Vanden Bossche, the COVID jabs, from the beginning, have produced the wrong immune response, which inevitably leads to immune escape. In summary, when you vaccinate against one variant, in this case the original Wuhan strain, your immune system will produce antibodies against that strain.
When your immune system is then hit with a second variant — as is the case when the vaccine is a step behind — it will be overly focused on the original strain, which allows the second strain to pass through its defenses.
Vanden Bossche’s concern now is the possibility of variants capable of causing more severe symptoms. We haven’t seen that yet, but as he notes in this interview, the mutations are no longer limited to conserved domains shared by many variants, but are also found in other viral proteins, some of which may enhance infection.
He goes on to explain a vaccinology concept called “immune refocusing,” which is how more dangerous viruses can be created. Immune refocusing happens when you have a vaccine breakthrough infection, meaning the vaccine did not result in enough neutralizing antibodies to block the virus. This is also known as a “leaky vaccine.”
The breakthrough infection boosts production of previously induced antibodies, giving you very high titers. And, while they have very low neutralizing capacity, the sheer number of them can still have some neutralizing, albeit short-lived, effect on the virus.
During the time the antibodies have this neutralizing effect, they bind to the dominant epitopes (an epitope is the part of the antigen that is recognized by your immune system), and by doing so, the subdominant epitopes that normally are outcompeted by the dominant ones can now be recognized by your immune system.
By continuing with boosters, we accelerate immune escape. Over time, variants will get better and better at evading our immune responses, and those who keep taking boosters will be the most vulnerable to infection of all.
The problem is that once these antibodies begin to lose their neutralizing capacity, they become sub-neutralizing, which allows for the propagation of more infectious variants. The mRNA jabs make immune refocusing all the more likely because they induce antibodies with low affinity to the immunodominant epitopes from the start, and automatically prioritize subdominant epitopes. This, Vanden Bossche explains, is why:
“… after the second dose of mRNA vaccine, we have seen cross-neutralizing antibodies against several different variants. Of course the manufacturers and the WHO were saying, ‘Oh wow, this is great … We are now broadening the immune response.’
[But] they have not taken into account that they [are] generating low-affinity antibodies and that is why they … very rapidly evolve toward sub-neutralization, suboptimal titers that … drive immune escape.”
The key take-home from all of this is that our immune response will never get any better if we continue this way. In fact, by continuing with boosters, all we’re doing is accelerating immune escape, Vanden Bossche warns. Over time, the variants will get better and better at evading our immune responses, and those who keep taking boosters will be the most vulnerable to infection of all.
This is the exact opposite of what vaccination is all about, and could result in an absolute public health disaster, especially should variants also begin to mutate into strains that cause more serious symptoms.
What Concerns Vanden Bossche About JN.1
While JN.1 does not appear to be any more troublesome than previous variants, Vanden Bossche worries about what this particular variant tells us about the immune pressures that gave rise to it in the first place.
The neutralizing domains of the spike protein have completely changed from the original. They’re even completely different from BA.2, from which JN.1 arose, as shown in a November 2023 study in the journal Vaccine.10
The problem, Vanden Bossche explains, is that while vaccine developers point to high titers of neutralizing antibodies against various variants (including JN.1) at two weeks post-jab, they’re ignoring (or hiding) the fact that these are not true neutralizing antibodies. Vanden Bossche refers to them as pseudo-neutralizing, because:
“… they have no specificity for the monovalent epitope. They can only interact with the multimeric presentation of the spike on a viral particle, or on viral aggregates, and therefore their neutralizing effect is very much limited in time, and that is … what JN.1 tells us.
JN.1 is fine in its own right, but it tells us something which is extremely worrisome. It tells us, basically, that the highly vaccinated populations have … progressed their antibodies to stabilizing aggregates that are now primarily taken up by antigen-presenting cells and are driving mitigation of infection, because even vaccinees [vaccine recipients] who are regularly exposed have no severe symptoms …
The vast majority of regularly exposed have, still, relatively mild symptoms, so mitigation of the disease is now explained by the cytotoxic T cells that will abrogate infection, or kill cells that have been infected … That is another way of mitigating the infection, which is driving … more infectious variants like JN.1 …
We see that JN.1 spreads like wildfire. It has outpaced all of the co-circulating variants globally in no time … Secondarily, we see a very clear surge in cases of hospitalization, severe disease and death … in several European countries …
But the most interesting thing, when you look at the changes in JN.1 … there is something extremely spectacular. For the first time, the mutations are no longer limited to conserved domains … those that are shared among several different variants. The mutations seen in JN.1 … are very uncommon.
We are also seeing a number of mutations that aren’t even spike specific anymore. They are located in other viral proteins, and these mutations have an infection-enhancing effect … They are, for example, promoting the efficiency of viral protein synthesis, or they are promoting the efficacy of intracellular viral replication …
What I see is that JN.1 is the result of immune pressure on the virus. An immune pressure that … moved away very clearly from targeting common epitopes that are shared among several different variants … and it moved away from targeting epitopes that are within the spike …
When you put all these things together, you can now clearly confirm that … we have been shifting the immune focusing from the humoral response to a cellular response … This immune refocusing is driven by antibodies of lower and lower affinity … What this means is … none of the updated vaccines will work …
Remember, every single time you have vaccine breakthrough infection, you boost [the pseudo-neutralizing antibodies], but … if this boosting effect no longer takes place, or is diminishing … then you will see a decline in those antibodies …
When the concentration diminishes … infection-enhancing antibodies are a disaster, because these infection-enhancing antibodies are also responsible for inhibiting the virulence of the virus … So now you are going to put suboptimal immune pressure on viral virulence, and that is what’s going on.”
The Jabbed Will Be at Grave Risk if SARS-CoV-2 Becomes More Virulent
Because of the mutations seen in JN.1, Vanden Bossche predicts we will “very soon” see variants that are more virulent, meaning more damaging and deadly. If this happens, healthy unjabbed individuals are unlikely to be affected, according to Vanden Bossche, because their first line of defense — their innate immune system — still works as it should.
As a virus becomes more virulent, it typically has to pay a fitness cost, so it becomes less infectious. In other words, it won’t spread as easily, but when it does infect someone, it causes more severe disease.
Vanden Bossche predicts that since the innate immune systems of the unjabbed have been continuously trained on all these different variants, they are therefore less likely to become infected, and if they do, they will be largely asymptomatic.
The jabbed, on the other hand, whose innate immune systems have not been trained, and whose adaptive immune systems have become increasingly useless thanks to the processes described by Vanden Bossche, will be at very high risk of severe complications and death.
mRNA Jab Causes Off-Target Effects
The latest COVID injections contain a single modified RNA said to correspond to the Omicron variant XBB.1.5., which was the dominant variant in the U.S. for most of 2023, but which has since been replaced by JN.1 and several other variants.
The SARS-CoV-2 virus mutates so quickly, there’s simply no way to keep up, let alone get ahead of it, and as explained above, this catch-up game is ultimately what puts pressure on the virus to mutate, and potentially into a more virulent form.
On top of that, we now also know that the shots are producing off-target proteins in 25% to 30% of recipients, and are contaminated with DNA, both of which have huge potential to cause harm. Until or unless they fix those problems, the risks are simply unacceptable, in my opinion.
But even if these issues were successfully fixed, we’re still facing a situation in which continued boosting will accelerate mutations that could eventually make the virus deadlier again, at least for those who have taken the shots.
It’s basically a death spiral, and the only way to end it is to stop taking boosters. There are no indications that our health authorities will protect the public by withdrawing the COVID shots, so it’s incumbent on each individual person to simply say no.
Got the Jab? Take Action to Safeguard Your Health
If you already got one or more jabs and now have concerns about your health, what can you do? First and foremost, never take another COVID booster, another mRNA gene therapy shot or regular vaccine. You need to end the assault on your system.
If you developed symptoms you didn’t have before your shot, I would encourage you to seek out expert help. At present, the Front Line COVID-19 Critical Care Alliance (FLCCC) seems to have one of the best treatment protocols for post-jab injuries. It’s called I-RECOVER and can be downloaded from covid19criticalcare.com.11
Dr. Pierre Kory, who cofounded the FLCCC, has transitioned to treating the vaccine injured more or less exclusively. For more information, see DrPierreKory.com. Dr. Peter McCullough is also investigating post-jab treatments, which you can find on PeterMcCulloughMD.com.
The World Health Council has also published lists of remedies that can help inhibit, neutralize and eliminate spike protein, which most experts agree is the primary culprit. I covered these in my 2021 article, “World Council for Health Reveals Spike Protein Detox.”+ Sources and ReferencesTODAY’S FREE ARTICLES
Mercola proudly supports these charities and organizations. View All
Charities & Organizations
More About Mercola.com
Disclaimer: The entire contents of this website are based upon the opinions of Dr. Mercola, unless otherwise noted. Individual articles are based upon the opinions of the respective author, who retains copyright as marked. The information on this website is not intended to replace a one-on-one relationship with a qualified health care professional and is not intended as medical advice. It is intended as a sharing of knowledge and information from the research and experience of Dr. Mercola and his community. Dr. Mercola encourages you to make your own health care decisions based upon your research and in partnership with a qualified health care professional. If you are pregnant, nursing, taking medication, or have a medical condition, consult your health care professional before using products based on this content.
If you want to use an article on your site please click here. This content may be copied in full, with copyright, contact, creation and information intact, without specific permission, when used only in a not-for-profit format. If any other use is desired, permission in writing from Dr. Mercola is required.
Terms & Conditions • Updated Privacy Policy
© 1997-2024 Dr. Joseph Mercola. All Rights Reserved.